
“Campaign food is always bad, but the food that goes onto that airplane is, like, just poison,” Kennedy said on the podcast, likely referring to Trump’s private airplane. “You have a choice between – you don’t have the choice, you’re either given KFC or Big Macs.”
— RFK, Jr. August 2024
First of all, it is NOT a pyramid. It is upside down, and looks more like a wedge. Stuff at the top in the 90’s was bad for your health; e.g. fats, while stuff at the base was good for you; e.g. bread. In 2026 whole grain bread is now at the “bad” bottom, which is sad for me; he who likes to soak up all that red meat juice now at the top.
2026

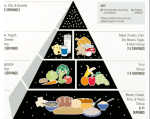
1992
When we interviewedRFK,Jr. for this blog, we asked why the pyramid had been turned upside down. He proudly responded, “The President wants us to change directions in every unexpected way possible”.
Milk has been so “bad” for our health for years that nutritionists, or at least dieters, parsed it into various levels of threat; regular, whole, 2%, 1%, skim, fat-free, lactose-free, and now soy, oat, cashew, and almond. The 2026 food guide puts whole milk and red meat right up there on top as “good”. In 2026 eggs remain on the second or third “good” level while nuts have dropped down several levels.
When asked which standard diet might be most consistent with the new food wedge, he answered, “The high protein KETO diet or PALEO (carnivore) diet, both of which are free of harvested grains. I admit they are hard to follow. I tried the PALEO diet once, but quit because I couldn’t always find saber tooth tiger steaks at Stop & Shop. My own preferred diet is ‘meat and ferments’.” When asked what he would bring to a Super Bowl party, he said, “I’d take a tub of yogurt and nutrient-dense whole food like road kill.”
He went on to position home cooking, with protein (presumably meat), as a remedy for what he called “spiritual malaise”: the loneliness, social fragmentation and suicidality among American youth. “We are engaged in spiritual warfare,” he said, “and the malevolent forces want to drive us apart.” He advised Americans to acquire cutting boards and cutlery.
When challenged about his credentials as a nutritionist he responded, “I refuse to explain my expertise when the next likely Surgeon General is currently a surgical resident with only a temporary medical license and no clinical practice experience . . . . although she does own or manages several supplement/wellness companies. So she might be very effective in getting Big Pharma lobbyists off our backs. Dealing with a bunch of lobbyists from the FDA-unregulated wellness/supplement companies might just be a breath of fresh air”.
“Big Food and Big Pharma have lied to us for decades about ‘essential’ nutrients,” RFK thundered. “Don’t you think it’s time to get all those specialty drugs ads – the ones with unpronounceable names lacking vowels — off the TV, and air some good MAHA ads for healthy ‘nutrient-dense whole foods’.”
One of RFK,Jr’s well known passions is the threat to our health from “ultra-processed” foods. The problem is:
“There is no universal definition of an ultra-processed food, and even experts don’t always agree about which foods count. Under the most commonly used definition ultra-processed foods are those made wholly or largely from oils, sugars, and starches with added emulsifiers or dyes. By that standard, classic “junk” foods like chips, candy, and soda are ultra-processed—but so are foods such as flavored yogurts, some whole-grain breads, and nondairy milks.”
I remember when a group of us medical residents were challenged by a very bright, obesity-expert physician to define “junk food”. He shot down our attempts very quickly with responses like: “Oh, high sugar and starch, like grandma’s apple pie”, etc. After twenty minutes of debate our only consensus that held up to his attacks was: “Junk food is that which is wrapped in cellophane and comes out of a vending machine”.
As our interview was ending we asked RFK, Jr. how the shoulder was feeling after his recent rotator cuff repair. He responded, “Just fine . . . and that nonsense on the web about an injury from the chin-up competitions with Hegseth and Kid Rock is absolutely false. I got all my childhood vaccinations in my left arm, and that shoulder has never been the same since.”
HAPPY APRIL FOOLS DAY



 Posted by hubslist
Posted by hubslist 